DUPIXENT is indicated in patients 6 years and older as add-on maintenance treatment for severe asthma with Type 2 inflammation characterised by:1
raised blood eosinophils (EOS)
and/or raised fraction of exhaled nitric oxide (FeNO)
who are inadequately controlled with high-dose (ages 12 and older) and medium-to-high dose (ages 6 to 11) inhaled corticosteroids (ICS) plus another medicinal product for maintenance treatment
DUPIXENT is an injectable biologic that inhibits both
IL-4 and IL-13 signalling1–3
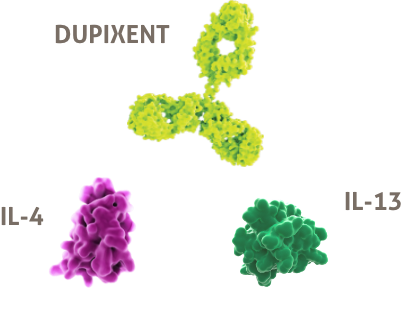
DUPIXENT is a biologic immunomodulator that targets more than one biomarker, unlike other available biologics1–3
 Biological therapies aim to alter the immunopathogenesis leading to asthma rather than manage the downstream airway inflammation3
Biological therapies aim to alter the immunopathogenesis leading to asthma rather than manage the downstream airway inflammation3
Other available biologics target either IgE or IL-5 whereas, DUPIXENT targets IL-4 and IL-31–3
What types of severe asthma patients can benefit from DUPIXENT?
The following criteria need to be met by your severe asthma patients:1
Patients 6 years and older with severe asthma
Patients with Type 2 inflammation, characterised by raised blood EOS and/or raised FeNO
Patients whose asthma is inadequately controlled with high-dose (ages 12 and older) and medium-to-high dose (ages 6 to 11) ICS plus another medicinal product for maintenance treatment
These severe asthma patients require treatment that will address their Type 2 patient profile

Illustrative patient profiles. Not actual patients.
INTRODUCING THE DUPIXENT PRE-FILLED PEN
DUPIXENT can be administered via
a pre-filled pen or a syringe1

![]()
Efficacy results
Learn more about how DUPIXENT can improve asthma in adults and adolescents.
- DUPIXENT Summary of Product Characteristics, Date last accessed: May 2023.
- Gandhi NA, et al. Nat Rev Drug Discov. 2016;15:35–50.
- Krings JG, et al. J Allergy Clin Immunol Pract. 2019;7(5):1379–1392.
- Peters MC, et al. J Allergy Clin Immunol. 2014;133(2):388–394.
- Doran E, et al. Front Med. 2017;4:139.
EOS, eosinophils; FeNO, fractional exhaled nitric oxide; ICS, inhaled corticosteroid; IL, interleukin.
References
MAT-XU-2204825 (v1.0) | Date of preparation: May 2023
