No single biomarker fully captures the complexity of
Type 2 inflammation in asthma1–6
50*–70%† of asthma patients have Type 2 inflammation1,2
Based on the Global Initiative for Asthma (GINA) guidelines, Type 2 inflammation is indicated by elevated levels of one or more of the following biomarkers:4,7
-
GINA recommends assessing the severe asthma phenotype during high-dose inhaled corticosteroids (ICS) treatment for evidence of Type 2 inflammation, including:
-
Blood eosinophils (EOS) ≥150 cells/µL
-
Asthma that is clinically allergen driven
-
Fractional exhaled nitric oxide (FeNO) ≥20 ppb
-
Need for maintenance oral corticosteroids (OCS)
-
Sputum EOS ≥2%
-
GINA recommends an add-on therapy (e.g. tiotropium, anti-IgE, anti-IL5/5R and anti-IL4R) for patients with exacerbations on a high-dose ICS/long-acting ß2-agonist (LABA) with or without daily OCS
-
FeNO
-
Blood EOS
-
Skin-prick test, IgE
- Maturation and differentiation driven by IL-5, trafficking to airway driven by IL-4 and IL-13
- Involved in maintaining long-term inflammation
- Associated with fixed airway obstruction
- Secretion induced by IL-4 and IL-13
- Associated with allergy
- Indicator of IL-13 driven inflammation
- Production induced by IL-4 and IL-13
- Indicator of corticosteroid responsiveness
- Useful in assessing asthma severity
Global and local guidelines
GINA8
BTS/SIGN4,7
BTS/SIGN recommend the options for investigation of eosinophilic inflammation or atopy are:
British Thoracic Society/Scottish Intercollegiate Guidelines Network (BTS/SIGN) guidelines recommend that omalizumab, mepolizumab, reslizumab and benralizumab may be considered in eligible patients with a high OCS burden
Type 2 biomarkers support the assessment of Type 2 inflammation9–12

EOS9–11

IgE9,10

FeNO9,12
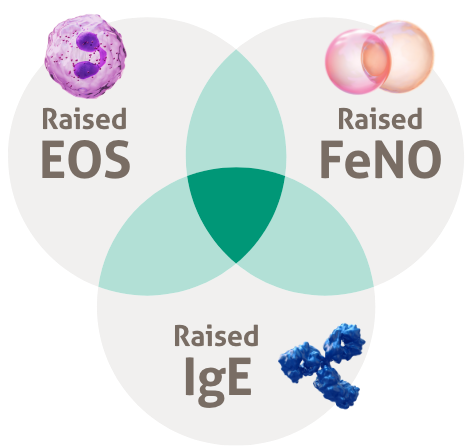
Multiple biomarkers and clinical information may be required to help select targeted therapies for patients with Type 2 inflammation in asthma5,6
The use of fractional exhaled nitric oxide (FeNO) and eosinophils (EOS) in combination may allow for better targeted and personalised treatment for severe asthma patients.6
Other available biologics target either IgE or IL-5 whereas, DUPIXENT targets IL-4 and IL-1313
Biological therapies aim to alter the immunopathogenesis leading to asthma, rather than manage the downstream airway inflammation.13
- Seys SF, et al. Respir Res. 2017;18:39.
- Peters MC, et al. J Allergy Clin Immunol. 2014;133(2):388–394.
- Peters MC, et al. J Allergy Clin Immunol. 2019;143(1):104–113.e14.
- GINA. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2020. Available at: https://ginasthma.org/severeasthma/. Date last accessed: May 2023 .
- Silkoff PE, et al. J Allergy Clin Immunol. 2017;140(3):710–719.
- Amaral R, et al. Clin Transl Allergy. 2018;8:13.
- GINA. Difficult-to-treat & severe asthma in adolescent and adult patients. A GINA Pocket Guide for Health Professionals. Available at: https://ginasthma.org/wp-content/uploads/2019/04/GINA-Severe-asthma-Pocket-Guide-v2.0-wms-1.pdf. Date last accessed: May 2023.
- BTS and SIGN (2019). SIGN 158. British guideline on the management of asthma. July 2019. Available at: https://www.sign.ac.uk/sign-158-british-guideline-on-the-management-of-asthma. Date last accessed: May 2023.
- Robinson D, et al. Clin Exp Allergy. 2017;47(2):161–175.
- Gandhi NA, et al. Nat Rev Drug Discov. 2016;15(1):35–50.
- Carr TF, et al. World Allergy Organ J. 2016;9:21.
- Alving K, et al. 2010. Exhaled Biomarkers (49)edn. Lausanne: European Respiratory Society, 1–31.
- Krings JG, et al. J Allergy Clin Immunol Pract. 2019;7(5):1379–1392.
- DUPIXENT Summary of Product Characteristics, Date last accessed: May 2023.
*Cluster analysis of sputum was done in asthmatic patients (n=205) and was defined as ‘cytokine-low/high’ if sputum mRNA expression of a particular cytokine was outside the respective 10th/90th percentile range of the control group (n=80). Half of patients (n=108; 52.6%) had a classical type 2 (TH2)-high (‘IL-4-, IL-5- and/or IL-13-high’) sputum cytokine profile.1 †The induced sputum cell pellets of asthmatic patients (n=37) and healthy control subjects (n=15) were examined to determine whether gene profiling in sputum cells can identify TH2-high and TH2-low subtypes of asthma. 70% (26/37) of the asthmatic patients had TH2-high asthma, which was characterised by more severe measures of asthma and increased blood and sputum eosinophilia.2
BTS, British Thoracic Society; EOS, eosinophils; FeNO, fractional exhaled nitric oxide; GINA, Global Initiative for Asthma; ICS, inhaled corticosteroids; IgE, Immunoglobulin E; IL, interleukin; IV, intravenous; LABA, long-acting ß2-agonist; OCS, oral corticosteroids; ppb, parts per billion; R, receptor; SC, subcutaneous; SIGN, Scottish Intercollegiate Guidelines Network; TH2, type 2.
References
MAT-GB-2004973 (v8.0) | Date of preparation: May 2023
