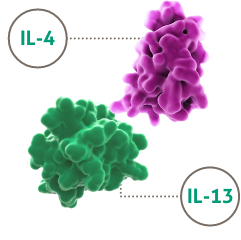
IL-4 and IL-13 are key drivers of Type 2 inflammation in severe asthma2–5
Patients with severe asthma risk mortality and corticosteroid-related morbidities6–9
Find out more >
DUPIXENT is a fully human monoclonal antibody that binds specifically to the IL-4Rα subunit and inhibits IL-4 and IL-13 signalling1
Find out more >
DUPIXENT is indicated in patients 6 years and older as add-on maintenance treatment for severe asthma with Type 2 inflammation characterised by raised blood eosinophils (EOS) and/or raised fraction of exhaled nitric oxide (FeNO), who are inadequately controlled with high-dose inhaled corticosteroids (ICS) plus another medicinal product for maintenance treatment1
No single biomarker fully captures the complexity of Type 2 inflammation in asthma3,4,10–13
DUPIXENT was studied in one Phase 2b and two Phase 3 clinical trials including 2,888 patients aged ≥12 years, with uncontrolled moderate-to-severe and severe asthma for up to 52 weeks1
![]()
The safety profile of DUPIXENT has been explored in the complexity of Type 2 inflammation in asthma, studied up to 1 year1
DUPIXENT can support your severe asthma patients:
 Adults, adolescents 12 years and older, and children aged 6-11 years old, as add on maintenance treatment for severe asthma
Adults, adolescents 12 years and older, and children aged 6-11 years old, as add on maintenance treatment for severe asthma
With Type 2 inflammation characterised by raised blood EOS and/or raised FeNO
Who are inadequately controlled with high-dose (12 years and older) and medium to high-dose (6 to 11 years) ICS plus another medicinal product or maintenance treatment.
.2022-01-31-12-09-21.png)
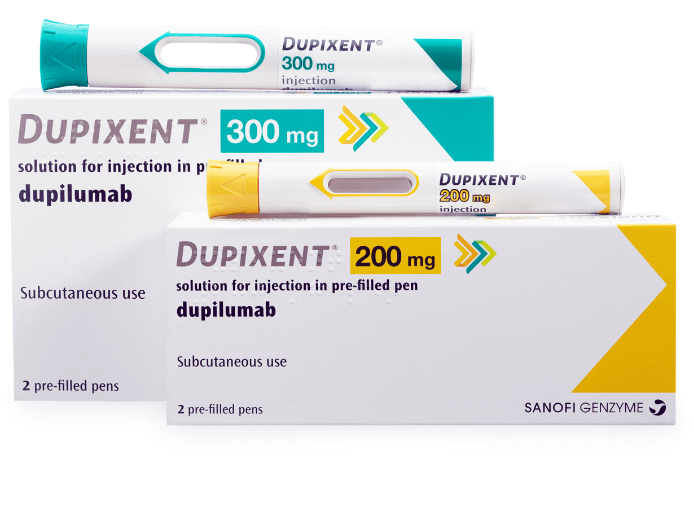
INTRODUCING THE DUPIXENT PRE-FILLED PEN
DUPIXENT can be administered via
a pre-filled pen or a syringe1
- DUPIXENT Summary of Product Characteristics. Date last accessed: May 2023.
- Tran TN, et al. Ann Allergy Asthma Immunol. 2016;116(1):37–42.
- Seys SF, et al. Respir Res. 2017;18:39.
- Peters MC, et al. J Allergy Clin Immunol. 2014;133(2):388–394.
- Doran E, et al. Front Med. 2017;4:139.
- Asthma UK (2017). Severe asthma: the unmet need and the global challenge. Available at: https://www.asthma.org.uk/globalassets/get-involved/external-affairs-campaigns/publications/severe-asthma-report/auk_severeasthma_2017.pdf. Date last accessed: May 2023.
- Asthma UK. What is severe asthma? Available at: https://www.asthma.org.uk/advice/severe-asthma/what-is-severe-asthma/#whatissevereasthma. Date last accessed: May 2023.
- Sweeney J, et al. Thorax. 2016;71(4):339–346.
- Why asthma still kills. The National Review of Asthma Deaths (NRAD). May 2014. Available at: https://www.rcplondon.ac.uk/projects/outputs/why-asthma-still-kills. Date last accessed: May 2023.
- Peters MC, et al. J Allergy Clin Immunol. 2019;143(1):104–113.e14.
- GINA. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2020. Available at: https://ginasthma.org/wp-content/uploads/2020/06/GINA-2020-report_20_06_04-1-wms.pdf. Date last accessed: May 2023.
- Amaral R, et al. Clin Transl Allergy. 2018;8:13.
- Silkoff PE, et al. J Allergy Clin Immunol. 2017;140(3):710–719.
- NICE guidance. Available at: https://www.nice.org.uk/guidance/indevelopment/gid-ta10276/documents/final-appraisal-determination-document. Date last accessed: May 2023.
EOS, eosinophils; FeNO, fractional exhaled nitric oxide; ICS, inhaled corticosteroids; IL, interleukin; OCS, oral corticosteroids; R, receptor.
References
MAT-GB-2004973 (v8.0) | Date of preparation: May 2023
__________________________________________________________________________________________________________________________________________________________________________
